Today I have a lot of information to share, and hope that you take the time to read through the material.
The link below to the Ovarian Cancer National Alliance reveals three studies that show the medical profession is still at odds as to the best screening tools for ovarian cancer. To me these findings are a little disappointing, only because we have to at least agree on the
I completely agree that unnecessary surgeries are a possible danger for some women, but overall, if a thorough evaluation is done before surgery, the risk would be minimal.
I say this because the insurance industry and medicare need to know what can be covered and make a difference. A real difference.
Medicare covers pelvic exams only once every 2 years. According to
approximately 46% of women diagnosed with ovarian cancer are age 65 or older. Think of all the women over 65 who will be diagnosed at an advanced stage because medicare doesn't cover this important screening tool more frequently!
I did not receive a bi-manual exam from my regular gynecologist and 5 months later I had Stage IIIC ovarian cancer and severe cervical dysplasia.
a few days ago. Our facilitator was genius, a woman from the Ovarian Cancer National Alliance. She kept talking about how important the bi-manual exam is and that it's "free". The students appeared so interested. I wonder if they were taken back though, like me. It's almost too simple. Sometimes we over-rely on technology........
This whole time I have been focusing on blood tests and trans-vaginal ultrasounds and CT scans. We need all of the above, but the bi-manual exam is so important. Our symptoms (see below) are primarily reflective of the displacement of the tissues and organs surrounding the ovaries, which is why interdisciplinary communication is SO important. Especially the GI doctors and the Gynecologists.
The facilitator was explaining that if the students know what normal ovaries feel like and where they are supposed to be, when they feel anything different, it can trigger them to look for more problems.
I never got the results of a trans-vaginal ultrasound that I had received about 10 months prior to diagnoses. I was refused a CA 125 because of having rheumatoid arthritis. I was told three times I was too young to have ovarian cancer. If any of these people would have been aware of the basics, including the doctor who didn't even do a bi-manual exam, my ovarian cancer would have been caught in an earlier stage.
For women, early stage diagnoses of ovarian cancers can mean longer survival rates. I try not to cling to statistics, but this is just common sense.
So if you are a medical student, please try to attend a Survivors Teaching Students presentation in your area. It will make a big difference in the number of lives you save. I was so honored to have a chance to share my story and the beautiful souls who participate in this program are just amazing. I am so grateful to have had this chance and look forward to more opportunities to meet these incredible students.
The students are incredible because when they go to a presentation such as this, you know that they really care about their responsibility. They are so busy, and that they took extra time to listen to us makes me feel good about their future.
Here is the link to the recent studies on what providers believe about ovarian cancer screening:
Ovarian cancer will be diagnosed in about one out of 55 women (approximately 1.8%). Ovarian cancer counts for about 3% of all cancers in women.
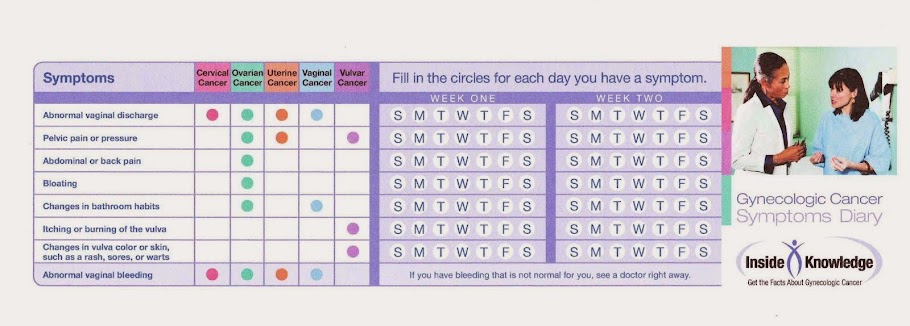
Ovarian cancer symptoms are often not taken seriously because they are similar to other women’s bodily complaints. The signs of ovarian cancer include:
• A feeling of being bloated
• Vague abdominal and pelvic discomfort
• Gastrointestinal symptoms such as gas, nausea, indigestion
• Constipation, diarrhea, frequent urination
• Back pain and fatigue
• Discomfort during sex
• Vaginal bleeding
Although many women have these symptoms of ovarian cancer, they are often overlooked. If any of these ovarian cancer signs are experienced almost every day and persist for weeks, they could be an early warning of ovarian cancer and should be brought to your doctor’s attention. Gilda Radner had every one of these symptoms for over a year prior to her diagnosis. Early detection can make the difference. Over 70% of all women with ovarian cancer will not be diagnosed until the disease has spread beyond the ovary. This is because the symptoms of early ovarian cancer are often vague and can mimic other common medical problems.
Unfortunately, there is no simple reliable ovarian cancer test available to screen women. Women need to stay in touch with their bodies and report changes to their doctors, because early detection is crucial. In a recent study more than 81% of women diagnosed with ovarian cancer had one of these symptoms before diagnosis. The Gilda Radner Familial Ovarian Cancer Registry has been recommending for over two decades that women experiencing continued symptoms of ovarian cancer have a combination of ovarian cancer tests that include
• Pelvic examination
• Vaginal ultrasound
• CA125 test
A Pap smear does not detect ovarian cancer. It is a screening tool to detect cervical cancer.
Ovarian cancer is most common in women who have already gone through menopause. The average age for developing ovarian cancer is 61 years of age. In families with two or more diagnoses of ovarian cancer, the cancer can be diagnosed at earlier ages, most commonly in their 40s.
Ovarian cancer prognosis is best when the disease is found early. Over 70% of all women with ovarian cancer will not be diagnosed until the disease has spread beyond the ovary. This is because the symptoms of early ovarian cancer can be vague and mimic other common medical problems. For the small number of women who are fortunate enough to have their cancer diagnosed before it has spread beyond the ovary, the chance for cure is 85 to 90%. However, for the majority of women in whom the disease has spread beyond the ovary, the chance of living for five years after the diagnosis is between 20 and 25%.
Specific risk factors or ovarian cancer causes are not known, but risk factors that may increase your chances of getting ovarian cancer may include:
• High fat diet
• Never having children
• Infertility, or not having children until late in life
• Using infertility drugs but not becoming pregnant
• Starting your periods at a young age, or going through menopause at an older than average age
• Use of talcum powder on the genital area
• Caucasian race
• Have an Eastern European (Ashkenazi) Jewish background.
• Family history of ovarian cancer, breast cancer, or colon cancer
• Peronal history of breast, uterine or colon cancer
Of these ovarian cancer risk factors, the most significant is a family history of ovarian cancer and /or breast cancer (on either your mother’s side of the family or your father’s side of the family). Having one close relative with ovarian cancer increases a woman’s risk of developing ovarian cancer by nearly three times. Having additional family members with breast cancer, ovarian cancer or colon cancer increases the risk even further.
Most women with ovarian cancer risk factors will never actually get ovarian cancer. Even with significant factors such as family history, the overall chances of getting ovarian cancer are still small.
Fortunately, there are a number of factors that are associated with lowering the risk of ovarian cancer.
• Use of birth control pills
• Having multiple children
• Breast feeding
• Tubal ligation
• Having the ovaries removed (prophylactic oophorectomy)
If you have only one close relative, such as a mother or sister, with a history of ovarian cancer, the overwhelming chances are that you will not develop ovarian cancer. However, you are at increased risk, and special testing by your doctor may be indicated.
Once a year to every six months the Gilda Radner Familial Ovarian Cancer Registry recommends women who have at least one close relative with ovarian cancer have a
• Pelvic examination
• Vaginal ultrasound
• CA125 test
There are almost 40 different types of ovarian cancer. However, nine out of 10 ovarian cancer patients have epithelial tumors, which begin in the tissue of the surface of the ovary (epithelium). These are called adenocarcinomas – a malignant (cancerous) tumor of epithelial origin which begins in glandular tissue, Serous adenocarcinoma is seen most often, followed by endometrioid, mucinous and clear cell adenocarcinomas. Carcinomas of borderline malignancy are a subgroup of serous and mucinous adenocarcinomas, which are usually less aggressive and have a significantly higher cure rate than serous and mucinous adenocarcinomas.
The only definitive way to diagnose ovarian cancer is surgery to remove the tumor for laboratory evaluation. Fortunately, there are tests to help determine if surgery is needed. In addition to a pelvic exam, pelvic and vaginal ultrasound of the ovaries can often (but not always) help distinguish between malignant and benign (noncancerous) tumors. Cystic tumors (i.e., no solid areas suggesting cancer) are usually benign. When solid areas are seen on ultrasound, the chances of cancer increase. CA125 levels (a tumor marker in the blood), which are elevated in eight out of 10 women with advanced (stage III and stage IV) disease and in one out of two women with cancer localized in the ovary (stage I), can be determined by a simple blood test. However, CA125 levels can also be elevated in benign conditions – endometriosis, pelvic inflammatory disease of the tubes and ovaries, uterine fibroids, pregnancy – and sometimes in cancer of the pancreas and the gastrointestinal tract.
Stage refers to how far the disease has advanced. Accurate staging is important in treatment planning because the prognosis (outcome) worsens as the stage increases. Generally, there are four stages of ovarian cancer.
Stage I: The Cancer is limited to the ovary or ovaries
* Stage IA: The tumor is limited to inside of one ovary
* Stage IB: The tumor is limited to the inside of both ovaries
* Stage IC: The tumor is limited to one or both ovaries. In addtion, it appears on the surface of the ovary, a fluid-filled capsule
has burst or cancer cells are found in the abdominal fluid.
Stage II: The cancer is one or both ovaries and has spread to other parts of the pelvis.
* Stage IIA: The tumor has spread to the uterus, fallopian tubes or both
* Stage IIB: The cancer has spread to the bladder, rectum or colon
* Stage IIC: The cancer tumor has spread to any of the above. Also, it appears on the surface of the ovary, a fluid-filled capsule
has burst or cancer cells are found in the abdominal fluid.
Stage III: The cancer is in one or both ovaries and has spread to nearby lymph nodes or other abdominal organs, not including the liver
* Stage IIIA: The tumor has spread to the lining of the abdomen but cannot be seen. The cancer has not spread to the lymph
nodes
* Stage IIIB: The cancer has sprread to the abdomen and is visible (less than two centimeters, about 3/4 of an inch in size).
The cancer has not spread to the lymph nodes.
* Stage IIIC: The cancer has spread into the abdomen and the deposits measure largers than two centimeters. The cancer has
spread to the lymph nodes.
Stage IV: The cancer has spread to the lung, liver or other distant organs.
Recurrent Ovarian Cancer: The cancer has come back after it has been treated. It may appear in other parts of the body, but is still considered ovarian cancer.
Surgery is needed for all stages of ovarian cancer, and when the surgeon (gynecologic oncologist) can document that cancer is limited to the ovary, it may be the only treatment needed. To document this, four areas within the abdominal cavity are evaluated: 1) the under-surface of the diaphragm; 2) the omentum (a fatty apron that hangs down from the colon); 3) lymph nodes along the abdominal aorta; and 4) pelvic lymph nodes. The abdominal cavity is also washed with a saline solution and the cells are stained to identify floating cancer cells not visible to the naked eye. For stages II, III, and IV, maximal tumor removal, ideally when surgery is performed by a gynecologic oncologist, results in the best survival rate.
Most women will get chemotherapy. The most important chemotherapy (drug treatment) agents for ovarian cancer are Platinum compounds and Taxanes. These medications are usually given intravenously (through a vein) every three to four weeks, for six treatments. Patients are evaluated at each treatment and have a pelvic examination, C125 test and blood work. If the CA125 level was elevated before, and is falling during chemotherapy, the treatment is almost certainly effective. If the CA125 level rises significantly during chemotherapy, it usually means that the treatment is not effective. Some women receive intra-peritoneal chemotherapy (through a small catheter inserted into their abdominal [peritoneal] cavity). Intraperitoneal chemotherapy is often used when only very small deposits of cancer remain within the abdominal cavity after primary surgery.
There are other promising chemotherapy drugs available. Topotecan, Gemcitabine, Hexamethylmelamine, Tamoxifen, Doxil, or oral etoposide are effective in some women. In some patients, newer agents such as Avastin (an anti-angiogenic agent), are used to cut off blood supply to the tumor.
The BRCA1 and BRCA2 genes are responsible for many cases of familial ovarian cancer and familial breast cancer. Genes are small pieces of DNA, the material that acts as a master “blueprint” for all the cells in your body. Your genes determine such things as what color hair and eyes you have, how tall you are, and what you look like on the inside. They also instruct the body how to build all the chemical substances in your body that keep you running smoothly. Sometimes there is an error in one of your genes that causes it not to do its job properly. This can lead to disease and is called a “genetic defect”.
The BRCA1 and BRCA2 genes make a chemical substance that helps your body prevent cancer. Most women have two normal copies of the BRCA1 gene, or BRCA2 gene both of which produce this cancer preventing substance. Some women have a genetic defect in one of their two BRCA1 genes or BRCA2 genes and don’t produce a normal amount of this cancer fighting substance. These women are at very high risk of getting breast or ovarian cancer, as high as 85-90% over the course of a lifetime.
You inherit one copy of each of your genes from your mother and a second copy of each of your genes from your father. (This is why you look about half like your mother, and half like your father). If one of your parents has a defective BRCA1 gene or BRCA2 gene there is a 50% chance you may inherit their defective copy, and 50% chance you may inherit their normal copy. If you inherit a defective BRCA1 gene, or BRCA2 gene, then each of your children has 50% chance of inheriting it from you.
Although there is a test to detect a defective BRCA1 or BRCA2 gene, such a test is not recommended for all women. Women with a strong family history of ovarian cancer should consult their physicians about the test. It is best that genetic testing start with the family member diagnosed with cancer.
All women with a genetic mutation for BRCA1 or BRCA2 should consider removal of their ovaries after childbearing. For other women at high risk for ovarian cancer, because of a strong family history of ovarian cancer who choose not to undergo genetic testing or who do not carry a mutation for BRCA1 or BRCA2 should consider the surgery in a case by case basis. The removal of the ovaries (oophorectomy) can be accomplished as a simply outpatient surgery using a device called a laparoscope. There is only minimal discomfort, and in most cases a woman can return to work in two to three days. Because there is still a small risk of a similar type of cancer of the lining of the abdominal cavity, called primary peritoneal cancer, women who have their ovaries removed should continue to be seen by a doctor every six months and should continue routinely have the CA125 blood test. Women who have had their ovaries removed may want to continue on hormone replacement therapy (HRT), but need to take a cautious approach, in consultation with her own physician, due to the recent findings from the Women’s Health Initiative.
Women who have two or more close relatives diagnosed with ovarian cancer are asked to join the Gilda Radner Familial Ovarian Cancer Registry. By doing so, they can be assured of being kept informed of the very latest developments in familial ovarian cancer research. JOIN THE REGISTRY TODAY.
ABOUT THE REGISTRY
The Familial Ovarian Cancer Registry was established in 1981 by M. Steven Piver, M.D., former chairman of the Department of Gynecologic Oncology at Roswell Park Cancer Institute. In May 1990, the Registry was renamed to honor the memory of comedian, Gilda Radner, who died of ovarian cancer in 1989. Ms. Radner’s husband, film actor Gene Wilder, is honorary chairman of the Registry.
The Registry is a national computer tracking system that stores data for women with two or more close relatives who have been diagnosed with ovarian cancer and offers education, information and a Helpline with peer support for women at high risk (family history) of ovarian cancer.
The Gilda Radner Familial Ovarian Registry is pursuing research into causes of familial cancer in collaboration with investigators at Roswell Park Cancer Institute, Stanford University School of Medicine and Cambridge University. Our goals are to identify new genes associated with familial ovarian cancer, thereby improving genetic and psychosocial counseling for individuals and families and to characterize lifestyle choices (i.e., oral contraceptive use, hormone replacement therapy, number of pregnancies) that reduce ovarian cancer risk in women who may be more susceptible to the disease. We hope to acquire information that will lead to better methods for detecting ovarian cancer, for reliable predictive testing for cancer predisposition and ultimately, preventing the disease in future generations.
To date, the Registry has amassed the data for over 4,500 women who have been diagnosed with ovarian cancer in more than 1,850 families with two or more members with ovarian cancer.
Roswell Park Cancer Institute was founded in 1898 and is one of the oldest comprehensive cancer centers in the world. It is dedicated to providing total care for cancer patients, conducting research into the causes, treatment and prevention of cancer and to public and professional education.
Gilda Radner Familial Ovarian Cancer Registry
Roswell Park Cancer Institute
Elm and Carlton Streets
Buffalo NY 14263
1-800-OVARIAN
716-845-4503