http://m.whitehouse.gov/the-press-office/2014/08/29/presidential-proclamation-national-ovarian-cancer-awareness-month-2014
The White House
The White House
Office of the Press Secretary
For Immedtate Release
Presidential Proclamation National Ovarian Cancer Awareness Month, 2014
- - - - - - -
BY THE PRESIDENT OF THE UNITED STATES OF AMERICA
A PROCLAMATION
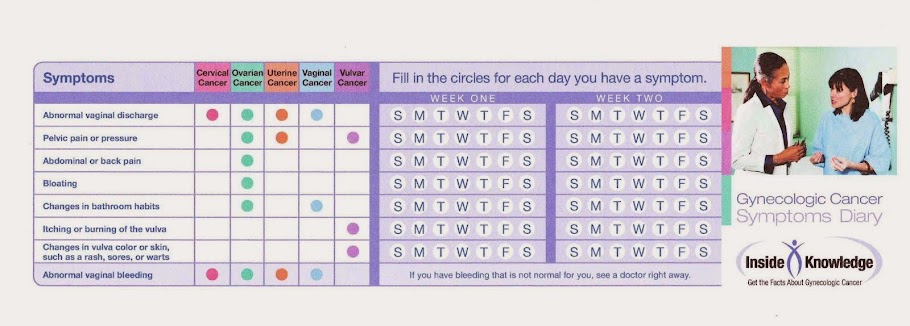
When ovarian cancer is found in its early stages, treatment is most effective and the chances for recovery are greatest. But ovarian cancer is difficult to detect early -- there is no simple and reliable way to screen for this disease, symptoms are often not clear until later stages, and most women are diagnosed without being at high risk. That is why it is important for all women to pay attention to their bodies and know what is normal for them. Women who experience unexplained changes -- including abdominal pain, pressure, and swelling -- should talk with their health care provider. To learn more about the risk factors and symptoms of ovarian cancer, Americans can visit www.Cancer.gov.
Regular health checkups increase the chance of early detection, and the Affordable Care Act expands this critical care to millions of women. Insurance companies are now required to cover well-woman visits, which provide women an opportunity to talk with their health care provider, and insurers are prohibited from charging a copayment for this service.
For the thousands of women affected by ovarian cancer, the Affordable Care Act also prohibits insurance companies from denying coverage due to a pre-existing condition, such as cancer or a family history of cancer; prevents insurers from denying participation in an approved clinical trial for any life-threatening disease; and eliminates annual and lifetime dollar limits on coverage. And as we work to ease the burden of ovarian cancer for today's patients, my Administration continues to invest in the critical research that will lead to earlier detection, improved care, and the medical breakthroughs of tomorrow.
Ovarian cancer and the hardship it brings have affected too many lives. This month, our Nation stands with everyone who has been touched by this disease, and we recognize all those committed to advancing the fight against this cancer through research, advocacy, and quality care. Together, let us renew our commitment to reducing the impact of ovarian cancer and to a future free from cancer in all its forms.
NOW, THEREFORE, I, BARACK OBAMA, President of the United States of America, by virtue of the authority vested in me by the Constitution and the laws of the United States, do hereby proclaim September 2014 as National Ovarian Cancer Awareness Month. I call upon citizens, government agencies, organizations, health care providers, and research institutions to raise ovarian cancer awareness and continue helping Americans live longer, healthier lives. I also urge women across our country to talk to their health care providers and learn more about this disease.
IN WITNESS WHEREOF, I have hereunto set my hand this twenty-ninth day of August, in the year of our Lord two thousand fourteen, and of the Independence of the United States of America the two hundred and thirty-ninth.
BARACK OBAMA

